* My column in BusinessWorld on October 03, 2019.


See also:

The Philippines’ public health sector is not a “deprived”
sector in terms of annual budget to fulfill various agencies’ functions and
mandates. There are three reasons why.
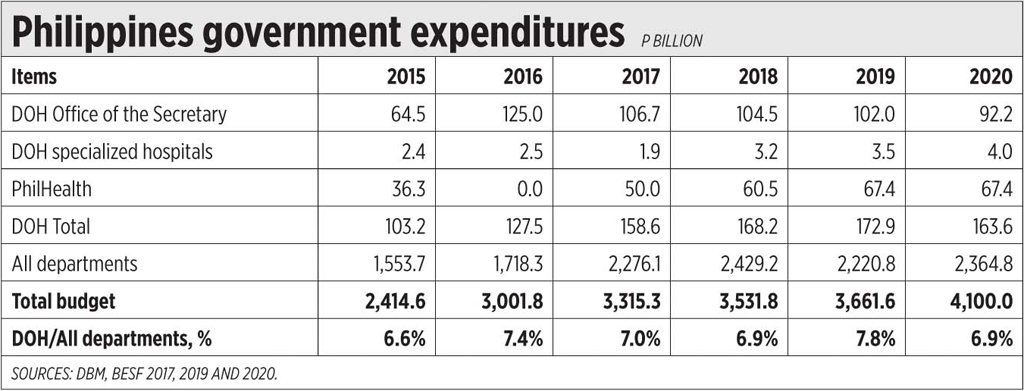
One, the annual budget of the Department of Health (DoH)
keeps rising and constitutes around 7% of total budgets by all departments, the
Legislative, and Judiciary. The data in the table comes from the Department of
Budget and Management (DBM), Budget of Expenditures and Sources of Financing
(BESF), submitted to Congress usually days after the President’s SONA.
Two, there are many other national agencies that also
provide public health services and subsidies, like the hospitals of state
universities including the University of the Philippines’ Philippine General
Hospital, hospitals by other agencies like Armed Forces of the Philippines
Hospital, Philippine National Police Hospital, plus health subsidies by
Philippine Amusement and Gaming Corp., Philippine Charity Sweepstakes Office,
and other national agencies.
Three, local government units (LGUs) have their own
provincial hospitals, or district hospitals, even city hospitals. Plus the
various barangay health centers, city and provincial centers.
If all the public spending by national government and
LGUs are combined, the Philippines would probably have at least 5% of GDP
minimum health spending.
Now the DoH has revived the drug price control policy,
officially called Maximum Retail Price (MRP), under the Cheaper Medicines Law
of 2008 (RA 9502).
In 2009, the DoH and Department of Trade and Industry
(DTI) jointly imposed the MRP, but because of heavy politicking that year
before the 2010 Presidential elections, they avoided using the term “MRP”
(which could mean “Mar Roxas for President”) and used “MDRP” (maximum drug
retail price) instead. Then they invented another term, GMAP (Government
mediated access price) to refer to “voluntary” price reduction. The subliminal
meaning of GMAP of course was Gloria Macapagal Arroyo Price. There was no
“health emergency” that year, only political emergencies for both the
administration and opposition.
The DoH Secretary that time was Francisco Duque. And he
is the DoH Secretary again now, and he is using the same political maneuvering
to impose drug price dictatorship again.
Luckily, the DTI Secretary now does not believe in
government price dictatorship and in arm-twisting innovator pharma companies to
bring down their prices or face huge penalties.
The DoH target now is 120 drugs that address leading
diseases and “catastrophic” conditions in the Philippines like hypertension,
diabetes, cardiovascular disease (CVD), chronic lung diseases, neonatal
diseases, and major cancers.
From the DoH press release, “Medicines were chosen on the
basis of burden of disease in terms of magnitude and the severity of the
conditions, high price arbitrage when compared with selected reference
countries, and the presence of limited competition.”
These are illegal criteria, not found in the law.
Under Section 7, Chapter 6 of the IRR, among the many
factors to consider in recommending MRP are the following:
“…Cost to the manufacturer, importer, trader,
distributor, wholesaler or retailer such as but not limited to: The exchange
rate of the peso to the foreign currency with which the drug or any of its
component, ingredient or raw material was paid for; Any change in the
amortization cost of machinery brought about by any change in the exchange rate
of the peso to the foreign currency with which the machinery was bought through
credit facilities; Any change in the cost of transporting or distributing the
medicines to the area of destination; Marketing Costs (per drug and total
global costs); Research Costs (local and global/per drug); Promotion Costs;
Advertising Costs; Incentives and Discounts; Taxes and other fees, impost,
duties, and other charges imposed by competent authority…”
These were not considered when price control was imposed
in 2009, and again not considered when price control will be imposed in 2019.
The DoH, as main implementer of RA 9502, becomes the chief violator of the
provisions of the law — not good.
If we want cheaper medicines, there are many factors that
government itself can do. Like reducing or abolishing import duties on
medicines, taxes and VAT on medicines. Have more competition among pharma
companies, innovators and generics, more competition among drug stores and
pharmacies, among hospitals. Not to mention, reduce government corruption in
the procurement of medicines.
The main function of government in this case is to ensure
the good quality of medicines, to go after manufacturers and sellers of fake,
counterfeit, and substandard medicines. Cheap but substandard medicines can
kill when the disease is not controlled and mutates to something more serious.
---------------See also:
The medicines offered by different alcohol rehab focuses vary from each other and they offer various kinds of directing meetings. In this manner, before picking a rehab, it is significant that every one of these things are mulled over. For example, there are guides to assist alcoholics with working through the issues that they have, there is bunch treatment that cause alcoholics to collaborate with different alcoholics and get support from others, etc.
ReplyDeleteoutpatient alcohol rehab florida